{kind=link}
{kind=link}
CMS published its 2007 physician fee schedule on August 22, after announcing it in June…
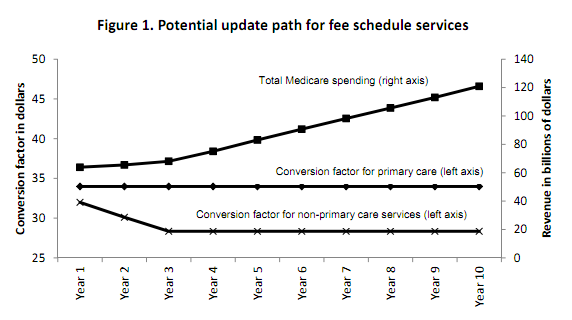
CMS issued the final MPFS — the Medicare Physician Fee Schedule for 2012 — this past week. The key feature of the rule, for many folks, is the Sustainable Growth Rate-(SGR)-mandated 27.4% cut in Medicare professional serivces reimbursements. We now get to watch the drama unfold over the next eight weeks, as the MedPAC proposal to replace the SGR is bandied about, and the machinations of the supercommittee tasked with brokering a budget fix either do or do not get us closer to a reasoned approach to doing more with less. The MedPAC idea is to drop the RBRVS conversion factor for specialty care payments 5.9% per year for two years, then hold it steady for 8 years, while keeping the primary care conversion factor flat for 10 years. The net effect: physician payments will "only" double over the next 10 years. (One clever idea squirreled away in the MedPAC report is that savings in the Medicare Shared Savings Plan (ACO) should be measured against a baseline of what Medicare would have spent on the care absent the changes in the proposed SGR fix — i.e., a higher baseline, with greater potential savings. Another 50 clever ideas like this and we'll be talking about saving some real money.)
Well, the SGR will be fixed (or not) by Congress, not CMS. The rest of the MPFS includes a variety of approaches to getting hands around the question of accuracy of the fee schedule. For example, per the CMS presser:
In addition, CMS is expanding the "potentially misvalued code initiative," an effort to ensure Medicare is paying accurately for physician services and more closely managing the payment system.
Finally, after struggling over time with varying requirements for lab test "requisitions" and "orders," which resulted in a CY 2010 requirement for a signed order prior to labs being drawn/done, CMS is backing off of that requirement, in response to comments detailing the ways in which this would reduce patient convenience and have the potential to negatively affect care.
Other issuances out the same day include the 2012 OPPS /ASC rule and the ESRD PPS rule.
David Harlow
The Harlow Group LLC
Health Care Law and Consulting
Healthcare NOW Radio Podcast Network · Harlow on Healthcare
In this episode I speak with Ryne Natzke, Chief Revenue Officer of TrustCommerce, a Sphere…
Natalie Davis, CEO of United States of Care, returned to Harlow on Healthcare to discuss…
If the EHR is the system of record, then Lumeon is the system of action.…
Blockchain in healthcare? Well, it can solve some problems. Have a listen to my conversation…
Joel Diamond, Chief Medical Officer at 2bPrecise, speaks with me about bringing genetic testing information…